Fill in a Valid Massachusetts Ta 1 Form
Fill in a Valid Massachusetts Ta 1 Form
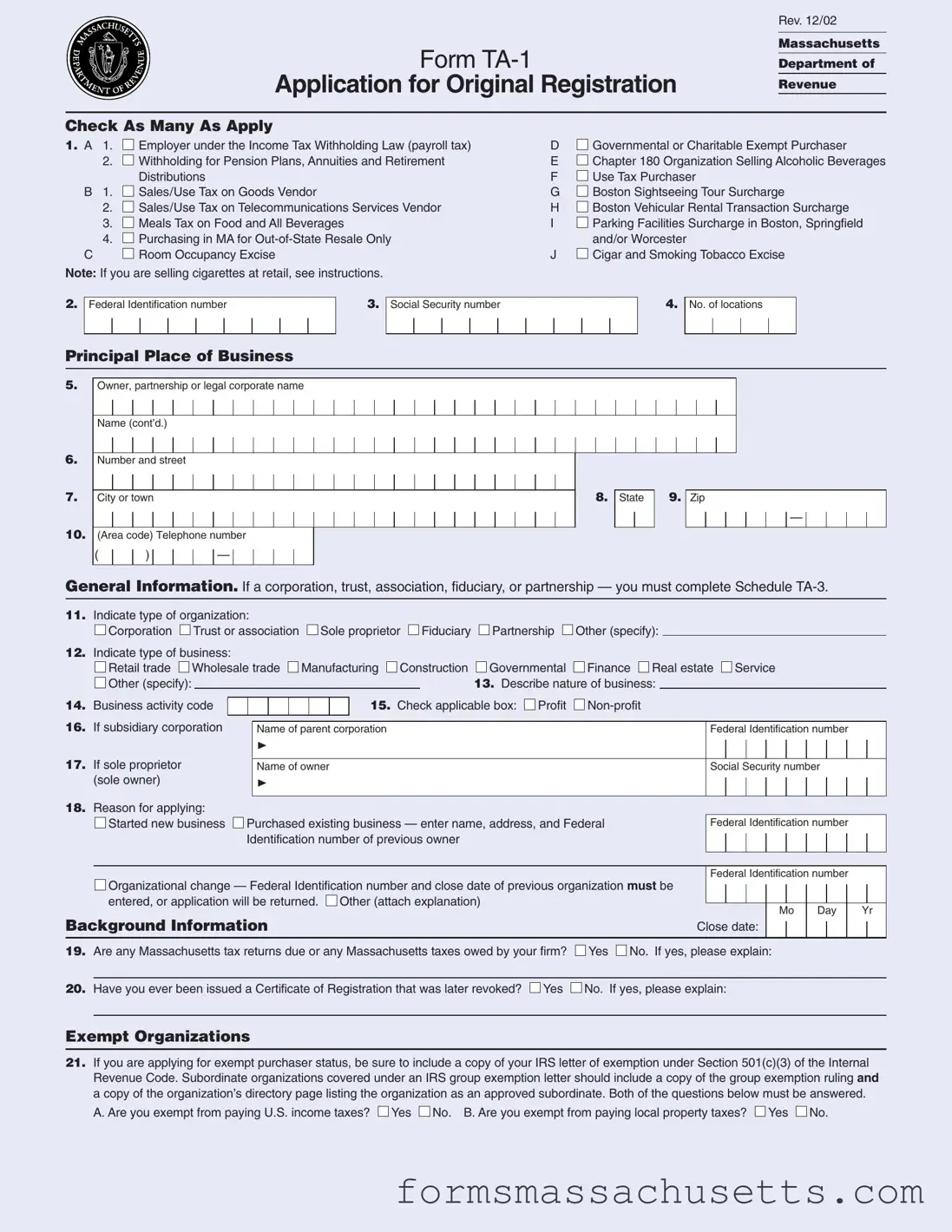
Starting a new business or changing the structure of an existing one can be an exciting yet daunting task. In Massachusetts, one of the essential steps in this process is completing the TA-1 form, which serves as an application for original registration with the Department of Revenue. This form is not just a bureaucratic requirement; it plays a crucial role in determining your business's tax obligations and compliance status. The TA-1 form covers a variety of important details, such as your business type—whether it's a corporation, partnership, or sole proprietorship—and the nature of your operations, from retail to manufacturing. Additionally, it requires you to specify your federal identification number, social security number, and any relevant tax history, including whether you owe any taxes or have had a registration revoked in the past. If your organization qualifies as a charitable entity, there are specific sections dedicated to exempt purchaser status, requiring documentation like your IRS exemption letter. Completing the TA-1 form accurately is vital, as it sets the foundation for your tax responsibilities and helps ensure that you’re operating within the legal framework of Massachusetts tax law.
Form
Application for Original Registration
Rev. 12/02
Massachusetts
Department of
Revenue
Check As Many As Apply
1. A |
1. |
|
Employer under the Income Tax Withholding Law (payroll tax) |
D |
|
Governmental or Charitable Exempt Purchaser |
|
|
|||||
|
2. |
|
Withholding for Pension Plans, Annuities and Retirement |
E |
|
Chapter 180 Organization Selling Alcoholic Beverages |
|
|
|
||||
|
|
|
Distributions |
F |
|
Use Tax Purchaser |
|
|
|
|
|||
|
|
|
|
|||
B |
1. |
|
Sales/Use Tax on Goods Vendor |
G |
|
Boston Sightseeing Tour Surcharge |
|
|
|||||
|
|
|||||
|
2. |
|
Sales/Use Tax on Telecommunications Services Vendor |
H |
|
Boston Vehicular Rental Transaction Surcharge |
|
|
|
||||
|
|
|
||||
|
3. |
|
Meals Tax on Food and All Beverages |
I |
|
Parking Facilities Surcharge in Boston, Springfield |
|
|
|
||||
|
|
|
||||
|
4. |
|
Purchasing in MA for |
|
|
and/or Worcester |
|
|
|
|
|||
|
|
|
||||
C |
|
|
Room Occupancy Excise |
J |
|
Cigar and Smoking Tobacco Excise |
|
|
|
||||
|
|
Note: If you are selling cigarettes at retail, see instructions.
2.
Federal Identification number
3.
Social Security number
4.
No. of locations
Principal Place of Business
5.
6.
7.
10.
Owner, partnership or legal corporate name
Name (cont’d.)
Number and street
City or town
(Area code) Telephone number
( |
|
) |
|
|
|
— |
|
|
|
|
8.
State
9.
Zip
—
General Information. If a corporation, trust, association, fiduciary, or partnership — you must complete Schedule
11.Indicate type of organization:

 Corporation
Corporation 
 Trust or association
Trust or association  Sole proprietor
Sole proprietor  Fiduciary
Fiduciary 
 Partnership
Partnership 

 Other (specify):
Other (specify):
12.Indicate type of business:
|
|
|
Retail trade |
|
|
Wholesale trade |
|
|
Manufacturing |
|
Construction |
|
|
Governmental |
|
|
Finance |
|
Real estate |
|
|
Service |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
Other (specify): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13. Describe nature of business: |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
14. |
Business activity code |
|
|
|
|
|
|
|
|
|
15. Check applicable box: |
|
Profit |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
16. |
If subsidiary corporation |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
Name of parent corporation |
|
|
|
|
|
|
|
|
|
|
|
|
|
Federal Identification number |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
❿ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
17. |
If sole proprietor |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
Name of owner |
|
|
|
|
|
|
|
|
|
|
|
|
|
Social Security number |
||||||||||||||||||||||||
|
(sole owner) |
|
|
|
|
❿ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
18. Reason for applying: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
Started new business |
|
Purchased existing business — enter name, address, and Federal |
|
Federal Identification number |
|
|
|||||||||
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
Identification number of previous owner |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Federal Identification number |
|
|
|||||||
|
|
|
Organizational change — Federal Identification number and close date of previous organization must be |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
entered, or application will be returned. |
|
Other (attach explanation) |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
Mo |
Day |
|
Yr |
|||||||
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Background Information |
Close date: |
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
19.Are any Massachusetts tax returns due or any Massachusetts taxes owed by your firm?  Yes
Yes  No. If yes, please explain:
No. If yes, please explain:
20.Have you ever been issued a Certificate of Registration that was later revoked?  Yes
Yes  No. If yes, please explain:
No. If yes, please explain:
Exempt Organizations
21.If you are applying for exempt purchaser status, be sure to include a copy of your IRS letter of exemption under Section 501(c)(3) of the Internal Revenue Code. Subordinate organizations covered under an IRS group exemption letter should include a copy of the group exemption ruling and a copy of the organization’s directory page listing the organization as an approved subordinate. Both of the questions below must be answered.
A. Are you exempt from paying U.S. income taxes?  Yes
Yes  No. B. Are you exempt from paying local property taxes?
No. B. Are you exempt from paying local property taxes?  Yes
Yes  No.
No.
Location of business |
Federal Identification number |
|
|
|
|
22.Trade name
Trade name (cont’d.)
23.Number and street (PO box is not acceptable)
24. |
City or town |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
25. |
State |
26. |
Zip |
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
27. |
(Area code) Telephone number |
|
|
|
28. |
Send certificate to: |
|
Principal place of business |
|
Location of business. |
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
( |
|
) |
|
|
|
— |
|
|
|
|
29. |
Send tax forms to: |
|
Principal place of business |
|
Location of business |
|
Other. |
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If “Other,” complete Schedule
Convention Center Financing District
30.Check here if your business location is within a Convention Center Financing District:  (see pages
(see pages
31.Check here if your business location is within a hotel, motel or other lodging establishment in Boston or Cambridge: 
Filing Frequencies
32. |
Is this location seasonal? (See instructions) |
|
|
Yes |
|
|
No. |
|
|
|
|
33. Indicate |
|||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||
|
If “yes,” check month(s) or partial month(s) business operates. |
|
|
|
|
|
|
paid for each applicable tax. Check the appropriate box(es). |
|||||||||||||||||||||||||||||||||||||||||||
|
Check month(s) |
Jan |
Feb |
Mar |
Apr |
May |
|
Jun |
|
Jul |
|
Aug |
Sep |
Oct |
Nov |
Dec |
Check appropriate box |
|
$0 – $100 |
$101– $1,200 |
over $25,000 |
||||||||||||||||||||||||||||||
|
Withholding |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Withholding |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Sales/Use on Goods |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Check appropriate box(es) |
|
|
|
$0 – $100 |
|
|
$101– $1,200 |
over $1,200 |
|||||||||||||
|
Sales/Use on |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sales/Use on Goods |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Telecom. Services |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sales/Use on Telecom. Services |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
Meals |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Meals |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Room Occupancy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Room Occupancy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Use Tax Purchaser |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Tax Type Information |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Withholding |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
34. |
Date you were first required to withhold |
|
Mo |
|
|
Day |
|
Yr |
|
|
|
|
|
35. Number of employees |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
taxes at this location. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
in Massachusetts: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Sales/Use Tax on Goods |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
36. |
Date you were first required to collect sales/use tax at this location. |
|
Mo |
|
Day |
|
Yr |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
Sales/Use Tax on Telecommunications Services |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
37. |
Date you were first required to collect sales/use tax on telecommunications services at this location. |
Mo |
Day |
|
Yr |
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||
Meals Tax on Food and All Beverages |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
38. |
Check if you serve: |
|
Food |
|
Beer |
|
|
Wine |
|
|
|
Alc. bev. |
|
|
|
|
39. Check if food/beverage vending machine: |
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
40. |
Date you were first required to collect meals tax. |
|
|
Mo |
|
|
Day |
Yr |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
41. Name and address
on liquor license42. Seating capacity: at this location.
Room Occupancy
43. |
Date you were first required to collect room occupancy tax. |
|
Mo |
Day |
Yr |
|
|
44. |
|
Locality code |
45. |
Number of rooms: |
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Use Tax Purchaser |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
46. |
Date you were first required to pay use tax. |
Mo |
|
Day |
|
|
Yr |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Convention Center Financing Surcharges |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
47. |
Date you were first required to collect: a. Boston Sightseeing Tour Surcharge. |
Mo |
Day |
|
Yr |
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
b. Boston Vehicular Rental Transaction Surcharge. |
Mo |
|
Day |
|
Yr |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
c. Parking Facilities Surcharge in Boston, Springfield and/or Worcester.
Mo
Day
Yr
Cigar and Smoking Tobacco Excise
48. Date you were first required to collect cigar and smoking tobacco excise. |
Mo |
Day |
Yr |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mail to: Massachusetts Department of Revenue, Data Integration Bureau, PO Box 7022, Boston, MA 02204.
I hereby certify that the statements made herein have been examined by me and are, to the best of my knowledge and belief, true and correct. Signed under the pains and penalties of perjury. The signing of this application is evidence that you may be individually and personally responsible for any sums required to be paid to the Commonwealth, under MGL, Chapters 62B, Sec. 5; 64G, Sec. 7B; 64H, Sec. 16 and 64I, Sec. 17.
Your signature
Title
Date
| Fact Name | Fact Description |
|---|---|
| Form Purpose | The TA-1 form is used for the application for original registration for various tax purposes in Massachusetts. |
| Governing Law | The form is governed by Massachusetts General Laws (MGL), specifically Chapters 62B, 64G, 64H, and 64I. |
| Exempt Purchaser Status | Organizations seeking exempt purchaser status must provide an IRS exemption letter under Section 501(c)(3). |
| Tax Types | The form covers various tax types, including sales/use tax, meals tax, and room occupancy excise. |
| Identification Numbers | Applicants must provide a Federal Identification Number and a Social Security Number. |
| Business Type | Applicants must indicate their type of organization, such as corporation, partnership, or sole proprietor. |
| Application Reasons | Common reasons for applying include starting a new business or purchasing an existing one. |
| Seasonal Operations | Applicants must indicate if their business location is seasonal, affecting tax filing frequency. |
| Tax Collection Dates | The form requires dates when the applicant was first required to collect various taxes. |
| Mailing Address | Completed forms should be mailed to the Massachusetts Department of Revenue, specifically the Data Integration Bureau. |
Massachusetts Form 3m - Through Form 3M, Massachusetts provides a structured way for non-profit entities to maintain tax compliance.
For more information on the process and to access the necessary documentation, you can visit Texas Documents, which provides a comprehensive guide to filling out the Texas Notice to Quit form correctly.
Lien Release Requirements by State - This document exemplifies the legal recourse available for unpaid work or materials, underpinning the concept of secured transactions.
Massachusetts Molst Form - The specificity of the form in regard to intubation and ventilation reflects an understanding of the complex nature of respiratory distress management.