Fill in a Valid Massachusetts Permit Electrical Form
Fill in a Valid Massachusetts Permit Electrical Form
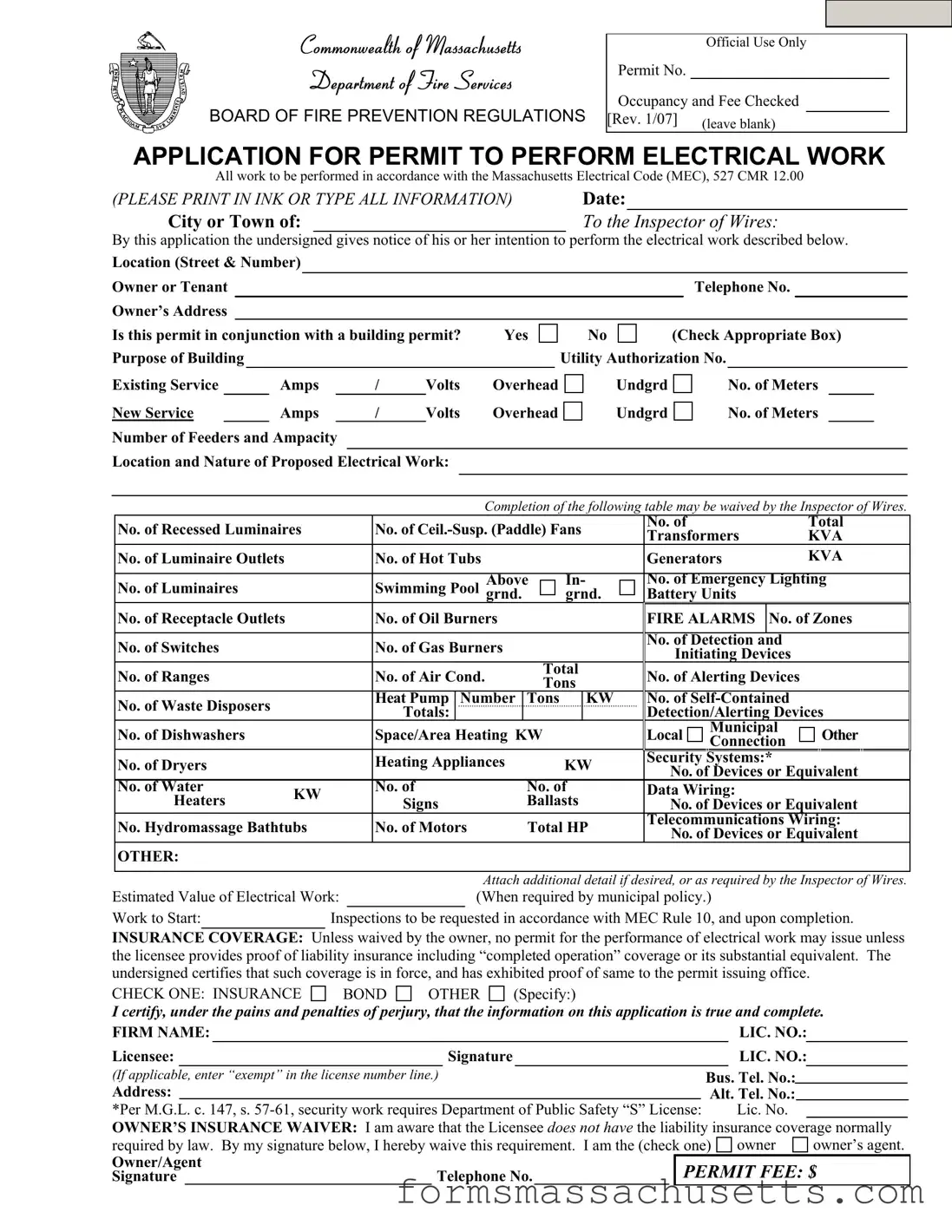
The Massachusetts Permit Electrical form is a critical document designed for those intending to perform electrical work within the Commonwealth. This application serves as a formal notice to the local Inspector of Wires, detailing the specific electrical tasks to be undertaken. Applicants are required to provide essential information, including the project’s location, the nature of the electrical work, and the estimated value of the project. The form also inquires about existing electrical services, such as amperage and voltage, and whether the permit is associated with a building permit. Additionally, it outlines various components of the electrical system, such as the number of luminaires, receptacles, and emergency lighting devices. To ensure compliance with local regulations, applicants must also confirm their liability insurance coverage, unless waived by the property owner. Furthermore, the form includes a section for workers' compensation insurance, emphasizing the importance of protecting both the workers and the project. By completing this form accurately and thoroughly, applicants facilitate a smoother permitting process and help uphold safety standards in electrical work.
Commonwealth of Massachusetts
Department of Fire Services
BOARD OF FIRE PREVENTION REGULATIONS
Official Use Only
Permit No.
Occupancy and Fee Checked
[Rev. 1/07] |
(leave blank) |
|
APPLICATION FOR PERMIT TO PERFORM ELECTRICAL WORK
All work to be performed in accordance with the Massachusetts Electrical Code (MEC), 527 CMR 12.00
(PLEASE PRINT IN INK OR TYPE ALL INFORMATION) |
Date: |
|
|
City or Town of: |
|
To the Inspector of Wires: |
|
By this application the undersigned gives notice of his or her intention to perform the electrical work described below.
Location (Street & Number) |
|
|
|
|
|
|
|
|
|
|||
Owner or Tenant |
|
|
|
|
|
|
|
|
|
Telephone No. |
|
|
Owner’s Address |
|
|
|
|
|
|
|
|
|
|
|
|
Is this permit in conjunction with a building permit? |
Yes |
No |
(Check Appropriate Box) |
|||||||||
Purpose of Building |
|
|
|
|
|
|
Utility Authorization No. |
|
||||
Existing Service |
Amps |
/ |
Volts |
Overhead |
Undgrd |
|
|
No. of Meters |
||||
New Service |
Amps |
/ |
Volts |
Overhead |
Undgrd |
|
|
No. of Meters |
||||
Number of Feeders and Ampacity
Location and Nature of Proposed Electrical Work:
Completion of the following table may be waived by the Inspector of Wires.
|
No. of Recessed Luminaires |
|
No. of |
No. of |
|
|
Total |
|||
|
|
Transformers |
|
KVA |
||||||
|
|
|
|
|
|
|
|
|||
|
No. of Luminaire Outlets |
|
|
No. of Hot Tubs |
|
|
Generators |
|
KVA |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
Above |
In- |
No. of Emergency Lighting |
||||
|
No. of Luminaires |
|
|
Swimming Pool grnd. |
|
grnd. |
Battery Units |
|
|
|
|
No. of Receptacle Outlets |
|
|
No. of Oil Burners |
|
|
FIRE ALARMS |
No. of Zones |
||
|
|
|
|
|
|
|
|
|
|
|
|
No. of Switches |
|
|
No. of Gas Burners |
|
|
No. of Detection and |
|
||
|
|
|
|
|
Initiating Devices |
|
||||
|
|
|
|
|
|
|
|
|||
|
No. of Ranges |
|
|
No. of Air Cond. |
Total |
No. of Alerting Devices |
|
|||
|
|
|
Tons |
|
||||||
|
|
|
|
|
|
|
|
|
||
|
No. of Waste Disposers |
|
|
Heat Pump Number |
Tons |
KW |
No. of |
|
||
|
|
|
Totals: |
|
|
Detection/Alerting Devices |
||||
|
|
|
|
|
|
|||||
|
No. of Dishwashers |
|
|
Space/Area Heating KW |
|
Local |
Municipal |
Other |
||
|
|
|
|
Connection |
||||||
|
|
|
|
|
|
|
|
|
||
|
No. of Dryers |
|
|
Heating Appliances |
|
KW |
Security Systems:* |
|
||
|
|
|
|
No. of Devices or Equivalent |
||||||
|
|
|
|
|
|
|
||||
|
No. of Water |
KW |
|
No. of |
No. of |
Data Wiring: |
|
|
||
|
Heaters |
|
Signs |
Ballasts |
No. of Devices or Equivalent |
|||||
|
|
|
||||||||
|
No. Hydromassage Bathtubs |
|
No. of Motors |
Total HP |
Telecommunications Wiring: |
|||||
|
|
No. of Devices or Equivalent |
||||||||
|
|
|
|
|
|
|
||||
|
OTHER: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
Attach additional detail if desired, or as required by the Inspector of Wires. |
||||||
Estimated Value of Electrical Work: |
(When required by municipal policy.) |
|
|
|||||||
Work to Start: |
|
Inspections to be requested in accordance with MEC Rule 10, and upon completion. |
||||||||
INSURANCE COVERAGE: Unless waived by the owner, no permit for the performance of electrical work may issue unless the licensee provides proof of liability insurance including “completed operation” coverage or its substantial equivalent. The undersigned certifies that such coverage is in force, and has exhibited proof of same to the permit issuing office.
CHECK ONE: INSURANCE |
BOND |
OTHER |
(Specify:) |
I certify, under the pains and penalties of perjury, that the information on this application is true and complete.
FIRM NAME: |
|
|
|
|
|
LIC. NO.: |
||||
|
|
|
|
|
|
|
|
|
|
|
Licensee: |
|
|
Signature |
|
|
LIC. NO.: |
||||
|
|
|
|
|
|
|
|
|
|
|
(If applicable, enter “exempt” in the license number line.) |
|
|
|
Bus. Tel. No.: |
||||||
Address: |
|
|
|
|
Alt. Tel. No.: |
|
|
|||
*Per M.G.L. c. 147, s. |
|
Lic. No. |
||||||||
OWNER’S INSURANCE WAIVER: I am aware that the Licensee does not have the liability insurance coverage normally
required by law. By my signature below, I hereby waive this requirement. I am the (check one) owner |
owner’s agent. |
||
Owner/Agent |
|
PERMIT FEE: $ |
|
Signature |
Telephone No. |
||
The Commonwealth of Massachusetts
Department of Industrial Accidents
Office of Investigations
600 Washington Street
Boston, MA 02111
www.mass.gov/dia
Workers’ Compensation Insurance Affidavit: Builders/Contractors/Electricians/Plumbers
Applicant InformationPlease Print Legibly
Name (Business/Organization/Individual):______________________________________________________
Address:__________________________________________________________________________
City/State/Zip:_____________________________ Phone #:________________________________
Are you an employer? Check the appropriate box:
Type of project (required):
1.
 I am a employer with _________
I am a employer with _________
employees (full and/or
2.


 I am a sole proprietor or partner- ship and have no employees working for me in any capacity. [No workers’ comp. insurance required.]
I am a sole proprietor or partner- ship and have no employees working for me in any capacity. [No workers’ comp. insurance required.]
3.

 I am a homeowner doing all work myself. [No workers’ comp. insurance required.] †
I am a homeowner doing all work myself. [No workers’ comp. insurance required.] †
4.

 I am a general contractor and I have hired the
I am a general contractor and I have hired the
5.

 We are a corporation and its officers have exercised their right of exemption per MGL c. 152, §1(4), and we have no employees. [No workers’ comp. insurance required.]
We are a corporation and its officers have exercised their right of exemption per MGL c. 152, §1(4), and we have no employees. [No workers’ comp. insurance required.]
6.
 New construction
New construction
7.

 Remodeling
Remodeling
8.
 Demolition
Demolition
9.
 Building addition
Building addition
10.

 Electrical repairs or additions
Electrical repairs or additions
11.
 Plumbing repairs or additions
Plumbing repairs or additions
12.

 Roof repairs
Roof repairs
13.

 Other____________________
Other____________________
*Any applicant that checks box #1 must also fill out the section below showing their workers’ compensation policy information.
†Homeowners who submit this affidavit indicating they are doing all work and then hire outside contractors must submit a new affidavit indicating such.
‡Contractors that check this box must attached an additional sheet showing the name of the
I am an employer that is providing workers’ compensation insurance for my employees. Below is the policy and job site information.
Insurance Company Name:____________________________________________________________________________
Policy # or 

Job Site Address:
City/State/Zip:______________________
Attach a copy of the workers’ compensation policy declaration page (showing the policy number and expiration date).
Failure to secure coverage as required under Section 25A of MGL c. 152 can lead to the imposition of criminal penalties of a fine up to $1,500.00 and/or
I do hereby certify under the pains and penalties of perjury that the information provided above is true and correct.
Signature:Date:
Phone #:
Official use only. Do not write in this area, to be completed by city or town official.
City or Town: ___________________________________ Permit/License #_________________________________
Issuing Authority (circle one):
1.Board of Health 2. Building Department 3. City/Town Clerk 4. Electrical Inspector 5. Plumbing Inspector
6.Other ______________________________
Contact Person:_________________________________________ Phone #:_________________________________
| Fact Name | Details |
|---|---|
| Governing Law | The Massachusetts Electrical Code (MEC), 527 CMR 12.00 governs the electrical work permit. |
| Application Requirement | All applicants must submit a completed application to the Inspector of Wires before commencing electrical work. |
| Insurance Requirement | Proof of liability insurance, including completed operation coverage, is mandatory unless waived by the owner. |
| Permit Fee | A permit fee is required, the amount of which is specified on the application form. |
| Completion Timeline | Work must start within the timeline specified on the application, and inspections should be requested accordingly. |
| Owner's Insurance Waiver | Owners can waive the insurance requirement by signing the designated section of the application. |
| Occupancy Information | Applicants must provide occupancy details and whether the permit is related to a building permit. |
| Estimated Work Value | Applicants may need to provide an estimated value of the electrical work being performed. |
| Workers’ Compensation Affidavit | Applicants must complete a Workers’ Compensation Insurance Affidavit to confirm insurance coverage status. |
| Application Submission | All information must be printed in ink or typed, ensuring clarity and legibility for processing. |
Pca Handbook - Centralizes the process of requesting changes or supplies into one accessible document, improving administrative efficiency.
Schedule 3k-1 - Requires the signature of a general partner, attesting to the accuracy of the information under penalty of perjury.
For those looking to navigate the intricacies of real estate transactions, a thorough understanding of the Real Estate Purchase Agreement is vital. This document forms the foundation of the buyer-seller relationship, ensuring clarity and protection throughout the process. To explore this important form further, you can access the necessary Real Estate Purchase Agreement guidelines for Colorado transactions.
Massachusetts State Tax Form - The Massachusetts Department of Revenue requires detailed information about the business, including federal identification numbers and social security numbers for sole proprietors.