Fill in a Valid Massachusetts 127 Form
Fill in a Valid Massachusetts 127 Form
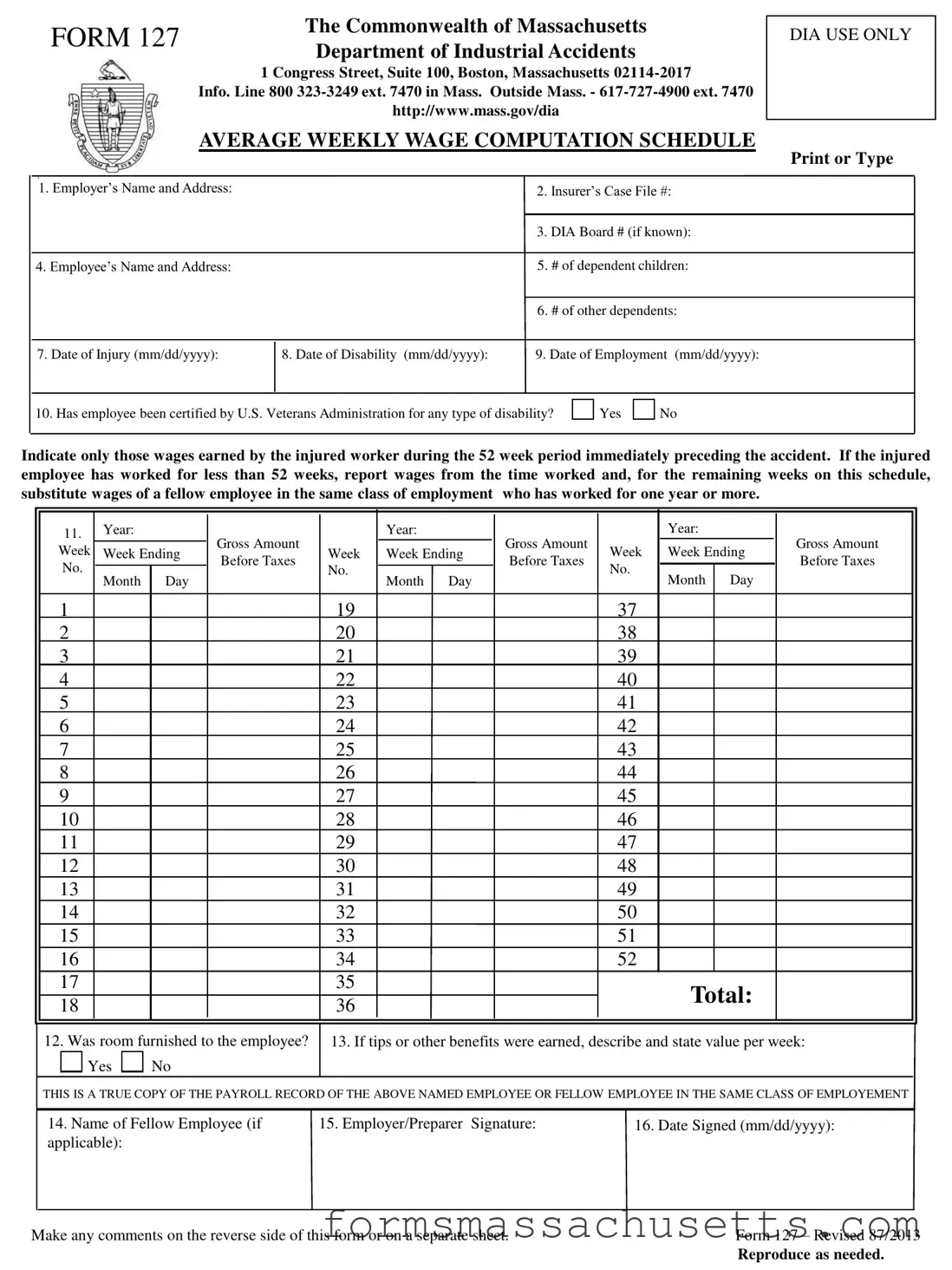
The Massachusetts 127 form plays a crucial role in the workers' compensation process, specifically for calculating an injured employee's average weekly wage. This form is utilized by the Department of Industrial Accidents and is essential for ensuring that employees receive fair compensation for lost wages due to work-related injuries. Key elements of the form include the employer's and employee's information, the dates of injury and disability, and the number of dependents. It requires a detailed account of the wages earned by the employee during the 52 weeks preceding the injury, with provisions for those who have worked for less than a year. Additionally, the form addresses whether any room or tips were provided to the employee, which can impact the overall wage calculation. Accurate completion of the Massachusetts 127 form is vital, as it directly influences the compensation benefits an injured worker may receive. Timeliness and precision in filing this form cannot be overstated, as delays or inaccuracies could result in significant financial hardship for the employee during their recovery period.
FORM 127 |
The Commonwealth of Massachusetts |
|
Department of Industrial Accidents |
||
|
||
|
1 Congress Street, Suite 100, Boston, Massachusetts |
|
|
Info. Line 800 |
|
|
http://www.mass.gov/dia |
|
|
AVERAGE WEEKLY WAGE COMPUTATION SCHEDULE |
DIA USE ONLY
Print or Type
1. Employer’s Name and Address: |
2. |
Insurer’s Case File #: |
|
|
|
|
3. |
DIA Board # (if known): |
|
|
|
4. Employee’s Name and Address: |
5. |
# of dependent children: |
|
|
|
|
6. |
# of other dependents: |
7. Date of Injury (mm/dd/yyyy):
8. Date of Disability (mm/dd/yyyy): |
9. Date of Employment (mm/dd/yyyy): |
10. Has employee been certified by U.S. Veterans Administration for any type of disability?
Yes
No
Indicate only those wages earned by the injured worker during the 52 week period immediately preceding the accident. If the injured employee has worked for less than 52 weeks, report wages from the time worked and, for the remaining weeks on this schedule, substitute wages of a fellow employee in the same class of employment who has worked for one year or more.
11. |
Year: |
|
|
Year: |
|
|
Year: |
|
|
||
|
|
|
|
|
|
||||||
Week |
Week Ending |
Gross Amount |
Week |
Week Ending |
Gross Amount |
Week |
Week Ending |
|
Gross Amount |
||
Before Taxes |
Before Taxes |
|
Before Taxes |
||||||||
No. |
Month |
Day |
|
No. |
Month Day |
|
No. |
Month |
Day |
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
|
|
19 |
|
|
37 |
|
|
|
|
2 |
|
|
|
20 |
|
|
38 |
|
|
|
|
3 |
|
|
|
21 |
|
|
39 |
|
|
|
|
4 |
|
|
|
22 |
|
|
40 |
|
|
|
|
5 |
|
|
|
23 |
|
|
41 |
|
|
|
|
6 |
|
|
|
24 |
|
|
42 |
|
|
|
|
7 |
|
|
|
25 |
|
|
43 |
|
|
|
|
8 |
|
|
|
26 |
|
|
44 |
|
|
|
|
9 |
|
|
|
27 |
|
|
45 |
|
|
|
|
10 |
|
|
|
28 |
|
|
46 |
|
|
|
|
11 |
|
|
|
29 |
|
|
47 |
|
|
|
|
12 |
|
|
|
30 |
|
|
48 |
|
|
|
|
13 |
|
|
|
31 |
|
|
49 |
|
|
|
|
14 |
|
|
|
32 |
|
|
50 |
|
|
|
|
15 |
|
|
|
33 |
|
|
51 |
|
|
|
|
16 |
|
|
|
34 |
|
|
52 |
|
|
|
|
17 |
|
|
|
35 |
|
|
|
Total: |
|
|
|
18 |
|
|
|
36 |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
12. Was room furnished to the employee?

 Yes
Yes 
 No
No
13. If tips or other benefits were earned, describe and state value per week:
THIS IS A TRUE COPY OF THE PAYROLL RECORD OF THE ABOVE NAMED EMPLOYEE OR FELLOW EMPLOYEE IN THE SAME CLASS OF EMPLOYEMENT
|
14. Name of Fellow Employee (if |
15. Employer/Preparer Signature: |
16. Date Signed (mm/dd/yyyy): |
|
|
applicable): |
|
|
|
|
|
|
|
|
Make any comments on the reverse side of this form or on a separate sheet. |
Form 127 – Revised 87/2013 |
|||
|
|
|
Reproduce as needed. |
|
Comments:
| Fact Name | Description |
|---|---|
| Purpose | The Massachusetts 127 form is used to calculate the average weekly wage for employees who have suffered a workplace injury. |
| Governing Law | This form is governed by Massachusetts General Laws Chapter 152, which pertains to workers' compensation. |
| Submission Requirements | Employers must complete the form with accurate wage information from the 52 weeks prior to the injury. |
| Dependent Information | The form requires information on the number of dependent children and other dependents of the injured employee. |
| Certification | It includes a question about whether the employee has been certified by the U.S. Veterans Administration for any type of disability. |
| Fellow Employee Wages | If the injured employee worked less than 52 weeks, wages of a fellow employee in the same job class may be used. |
| Signature Requirement | The form must be signed by the employer or preparer to certify the accuracy of the information provided. |
Form M-941 - Employers must sign the M-941A form, certifying the accuracy and completeness under penalties of perjury.
For those interested in navigating the property market, accessing the essential resources for a Real Estate Purchase Agreement can be invaluable. These agreements provide a structured framework for buyers and sellers to outline their terms clearly, enabling smoother transactions. You can find a detailed guide on this essential document at understanding the Real Estate Purchase Agreement process to better prepare for your real estate endeavors.
R109 - Applicants must provide a clear, legible photocopy of their ID if applying by mail.