Fill in a Valid 101 Massachusetts Form
Fill in a Valid 101 Massachusetts Form
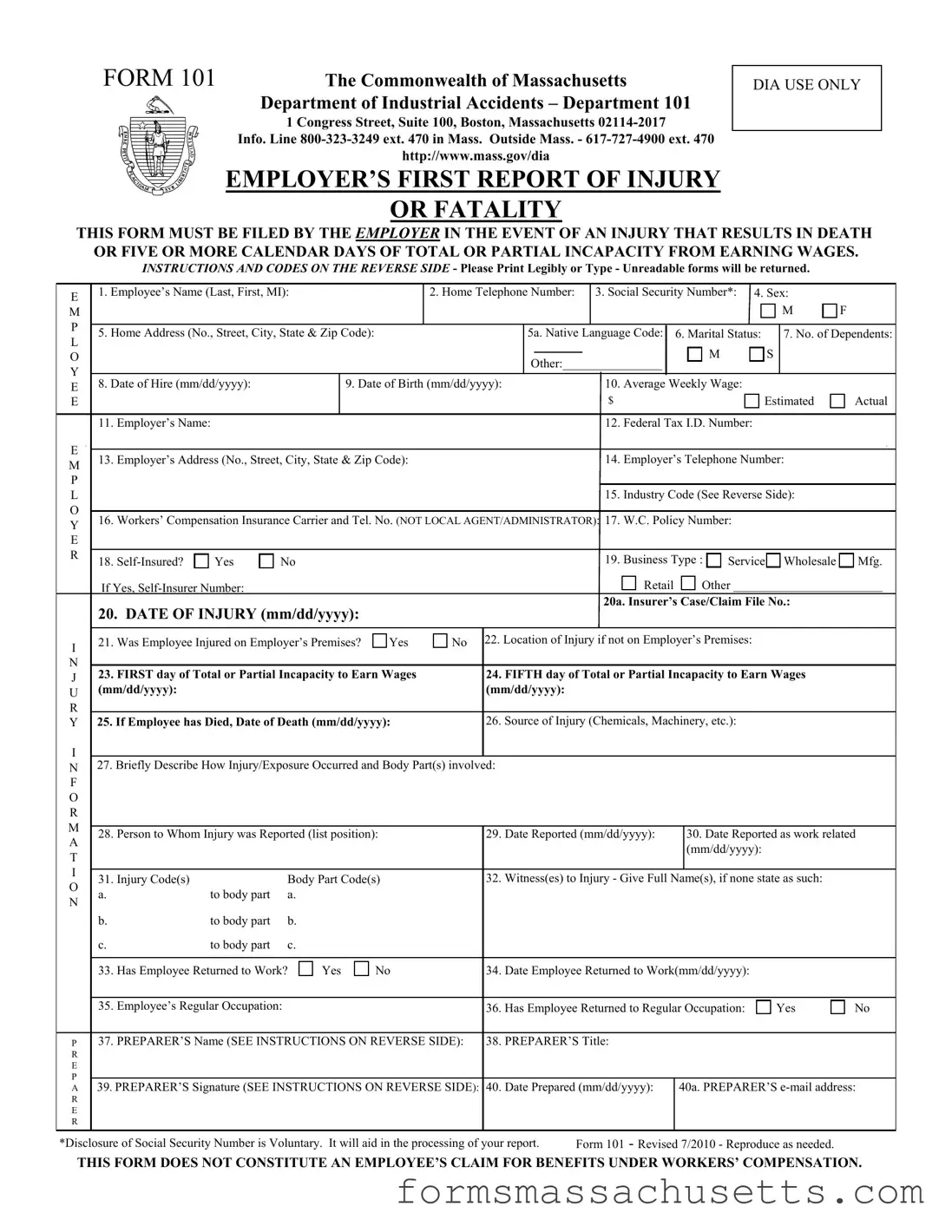
The 101 Massachusetts form, officially known as the Employer's First Report of Injury or Fatality, is a crucial document for employers in the Commonwealth of Massachusetts. This form must be submitted when an employee experiences an injury that leads to death or results in five or more calendar days of total or partial incapacity to earn wages. Its primary purpose is to ensure that the Department of Industrial Accidents is informed promptly about workplace injuries, allowing for appropriate follow-up and support for affected employees. The form requires detailed information about the injured employee, including their name, contact details, Social Security number, and employment specifics. Additionally, it captures essential data about the injury itself, such as the date it occurred, the nature of the injury, and whether it happened on the employer's premises. Employers are also required to provide information about their workers' compensation insurance and the circumstances surrounding the incident. Filing this form within seven calendar days is not just a procedural step; it is mandated by law, with penalties for non-compliance. Understanding how to accurately complete and submit the 101 Massachusetts form is vital for employers to fulfill their responsibilities and ensure that employees receive the necessary benefits and support following a workplace injury.
FORM 101 |
The Commonwealth of Massachusetts |
|
Department of Industrial Accidents – Department 101 |
|
1 Congress Street, Suite 100, Boston, Massachusetts |
|
Info. Line |
|
http://www.mass.gov/dia |
EMPLOYER’S FIRST REPORT OF INJURY
OR FATALITY
DIA USE ONLY
THIS FORM MUST BE FILED BY THE EMPLOYER IN THE EVENT OF AN INJURY THAT RESULTS IN DEATH OR FIVE OR MORE CALENDAR DAYS OF TOTAL OR PARTIAL INCAPACITY FROM EARNING WAGES.
INSTRUCTIONS AND CODES ON THE REVERSE SIDE - Please Print Legibly or Type - Unreadable forms will be returned.
E |
1. Employee’s Name (Last, First, MI): |
|
2. Home Telephone Number: |
3. Social Security Number*: 4. Sex: |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
|
|
M |
F |
P |
|
|
|
|
|
|
|
|
|
|
|
5. Home Address (No., Street, City, State & Zip Code): |
5a. Native Language Code: |
6. Marital Status: |
|
7. No. of Dependents: |
|||||||
L |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
O |
|
|
|
|
|
|
|
M |
S |
|
|
|
|
|
Other:________________ |
|
|
||||||
|
|
|
|
|
|
|
|||||
Y |
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
E |
8. Date of Hire (mm/dd/yyyy): |
9. Date of Birth (mm/dd/yyyy): |
|
|
|
10. Average Weekly Wage: |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
$ |
|
Estimated |
Actual |
|
|
11. Employer’s Name: |
|
|
|
|
|
12. Federal Tax I.D. Number: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
E |
13. Employer’s Address (No., Street, City, State & Zip Code): |
|
|
|
14. Employer’s Telephone Number: |
|
|||||
M |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
P |
|
|
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
15. Industry Code (See Reverse Side): |
|
|||
O |
|
|
|
|
|
|
|
|
|
|
|
Y16. Workers’ Compensation Insurance Carrier and Tel. No. (NOT LOCAL AGENT/ADMINISTRATOR): 17. W.C. Policy Number:
E
R |
18. |
Yes |
No |
|
19. Business Type : |
Service Wholesale |
Mfg. |
|
|
|
|||||||
|
If Yes, |
|
|
Retail |
Other ________________________ |
|||
|
|
|
|
|
20a. Insurer’s Case/Claim File No.: |
|
||
|
20. DATE OF INJURY (mm/dd/yyyy): |
|
|
|
|
|
||
I |
21. Was Employee Injured on Employer’s Premises? |
Yes |
No 22. Location of Injury if not on Employer’s Premises: |
|
||||
|
|
|
|
|
|
|
|
|
N |
|
|
|
|
|
|
|
|
J |
23. FIRST day of Total or Partial Incapacity to Earn Wages |
24. FIFTH day of Total or Partial Incapacity to Earn Wages |
|
|||||
|
|
|
|
|
|
|
|
|
U |
(mm/dd/yyyy): |
|
|
|
(mm/dd/yyyy): |
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
Y 25. If Employee has Died, Date of Death (mm/dd/yyyy): |
26. Source of Injury (Chemicals, Machinery, etc.): |
|
||||||
I
N27. Briefly Describe How Injury/Exposure Occurred and Body Part(s) involved:
F |
|
|
|
|
|
|
|
|
|
|
|
|
O |
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
|
|
|
|
M |
28. Person to Whom Injury was Reported (list position): |
|
29. Date Reported (mm/dd/yyyy): |
|
30. Date Reported as work related |
|||||||
|
|
|||||||||||
A |
|
|
||||||||||
|
|
|
|
|
|
|
|
|
(mm/dd/yyyy): |
|
|
|
T |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
31. Injury Code(s) |
|
Body Part Code(s) |
|
32. Witness(es) to Injury - Give Full Name(s), if none state as such: |
|
|||||||
O |
|
|
|
|||||||||
a. |
to body part |
a. |
|
|
|
|
|
|
|
|
|
|
N |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. |
to body part |
b. |
|
|
|
|
|
|
|
|
|
|
c. |
to body part |
c. |
|
|
|
|
|
|
|
|
|
|
33. Has Employee Returned to Work? |
Yes |
No |
|
34. Date Employee Returned to Work(mm/dd/yyyy): |
|
|
|||||
|
35. Employee’s Regular Occupation: |
|
|
|
|
36. Has Employee Returned to Regular Occupation: |
Yes |
No |
||||
P 37. PREPARER’S Name (SEE INSTRUCTIONS ON REVERSE SIDE): |
|
38. PREPARER’S Title: |
|
|
|
|
||||||
R |
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
P |
|
|
|
|
|
|
|
|
|
|
|
|
A 39. PREPARER’S Signature (SEE INSTRUCTIONS ON REVERSE SIDE): |
|
40. Date Prepared (mm/dd/yyyy): |
40a. PREPARER’S |
|||||||||
R |
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
|
|
|
|
*Disclosure of Social Security Number is Voluntary. It will aid in the processing of your report. |
Form 101 - Revised 7/2010 - Reproduce as needed. |
|
||||||||||
THIS FORM DOES NOT CONSTITUTE AN EMPLOYEE’S CLAIM FOR BENEFITS UNDER WORKERS’ COMPENSATION.
EMPLOYER’S FIRST REPORT OF INJURY OR FATALITY
FILING INSTRUCTIONS
1.WHEN TO FILE: File this form within 7 calendar days, not including Sundays and legal holidays, of receipt of notice of any injury alleged to have arisen out of and in the course of employment, which totally or partially incapacitates an employee for a period of 5 or more calendar days from earning wages. This form is not an admission of liability, but must be filed even though the Employer may believe that the Employee is not injured, or that the Employee is not entitled to benefits under M.G.L. Chapter 152.
2.WHERE TO FILE: This form should be mailed to the Department of Industrial Accidents at the address shown on the front of the form. Copies must also be provided to the Employee and to the Employer’s Workers’ Compensation insurer.
3.PENALTIES: Failure to report injuries on this form may result in a fine of $100.00 in accordance with M.G.L. Chapter 152, Section 6.
4.EMPLOYER’S NAME & SIGNATURE IN BOXES 37 & 39: This form must be filed by the employer or an authorized agent/representative of the employer.
NATIVE LANGUAGE CODES
1 – English / 2 – Portuguese / 3 – Haitian Creole / 4 – Spanish / 5 – Chinese / 6 – Vietnamese / 7 – Cape Verdean / 9 – Other
INDUSTRY CODES
Agriculture, Forestry and Fishing |
28 Chemicals and Allied Products |
51 Wholesale Trade - |
78 |
Motion Pictures |
||||
01 |
Agriculture Production - Crops |
29 |
Petroleum and Coal Products |
|
|
79 |
Amusements and Recreation Services |
|
02 |
Agriculture Production - Livestock |
30 |
Rubber and Misc. Plastic Products |
Retail Trade |
80 |
Health Services |
||
07 |
Agricultural Services |
31 |
Leather and Leather Products |
52 |
Building Materials and Garden Supplies |
81 |
Legal Services |
|
08 |
Forestry |
32 |
Stone, Clay and Glass Products |
53 |
General Merchandizing |
82 |
Educational Services |
|
09 |
Fishing, Hunting and Trapping |
33 |
Primary Metal Industries |
54 |
Food Stores |
83 |
Social Services |
|
Mining |
34 |
Fabricated Metal Products |
55 |
Automotive Dealers and Service Stations |
84 |
Museums, Botanical, Zoological Gardens |
||
35 |
Industrial Machinery and Equipment |
56 Apparel and Accessory Stores |
86 |
Membership Organizations |
||||
10 |
Metal Mining |
|||||||
36 |
Electronic and Other Electrical Equipment |
57 |
Furniture and Home Furnishing Stores |
87 |
Engineering and Management Services |
|||
12 |
Coal Mining |
|||||||
37 |
Transportation Equipment |
58 |
Eating and Drinking Establishments |
88 |
Private Households |
|||
13 |
Oil and Natural Gas |
|||||||
38 |
Instruments and Related Products |
59 |
Miscellaneous Retail |
89 |
Services, NEC |
|||
14 |
Nonmetallic Minerals, Except Fuels |
|||||||
39 |
Miscellaneous Manufacturing Industries |
|
|
|
|
|||
|
|
|
|
|
|
|||
Construction |
Transportation and Public Utilities |
Finance, Insurance and Real Estate |
Public Administration |
|||||
60 |
Depository Institutions |
91 |
Executive, Legislative and Garden |
|||||
15 |
General Building Contractors |
|||||||
40 |
Railroad Transportation |
|||||||
61 |
92 |
Justice, Public Order, and Safety |
||||||
16 |
Heavy Construction, Ex. Building |
|||||||
41 |
Local and Interurban Passenger Transit |
|||||||
62 |
Security and Commodity Brokers |
93 |
Finance, Taxation, and Monetary Benefits |
|||||
17 |
Special Trade Contractors |
|||||||
42 |
Trucking and Warehousing |
|||||||
63 |
Insurance Carriers |
94 |
Administration of Human Services |
|||||
|
|
|||||||
|
|
43 |
U.S. Postal Service |
|||||
Manufacturing |
64 |
Insurance Agents, Brokers and Service |
95 |
Environmental Quality and Housing |
||||
44 |
Water Transportation |
|||||||
20 |
Food and Kindred Products |
65 |
Real Estate |
96 |
Administration of Economic Program |
|||
45 |
Transportation by Air |
|||||||
21 |
Tobacco Products |
67 |
Holding and Other Investment Officers |
97 |
National Security and International Affairs |
|||
46 |
Pipelines, Except Natural Gas |
|||||||
22 |
Textile Mill Products |
|
|
|
|
|||
47 |
Transportation Services |
Services |
|
|
||||
23 |
Apparel and Other Textile Products |
|||||||
48 |
Communications |
70 Hotels and Other Lodging Places |
||||||
24 |
Lumber and Wood Products |
99 |
||||||
49 |
Electric, Gas and Sanitary Services |
72 |
Personal Services |
|||||
25 |
Furniture and Fixtures |
|
|
|||||
|
|
73 |
Business Services |
|
|
|||
26 |
Paper and Allied Products |
Wholesale Trade |
|
|
||||
75 |
Auto Repair Services and Parking |
|
|
|||||
27 |
Printing and Publishing |
|
|
|||||
50 |
Wholesale Trade - Durable Goods |
|
|
|||||
76 |
Miscellaneous Repair Services |
|
|
|||||
|
|
|
|
|||||
|
|
|
|
|
|
|||
NATURE OF INJURY OR ILLNESS CODES
100 |
Amputation or Enucleation |
157 |
Tuberculosis |
281 |
Aluminosis |
Other |
|
110 |
Asphyxia or Strangulation Etc. |
159 |
Other Infective or Parasitic Diseases |
282 |
Anthracosis |
265 |
Carpal Tunnel Syndrome |
120 |
Burns (Heat) |
Dermatitis |
283 |
Asbestosis |
510 |
Cardiovascular and Other Conditions |
|
130 |
Burns (Chemical) |
180 |
Dermatitis, UNS* |
284 |
Byssinosis |
|
of the Circulatory System |
140 |
Concussion |
183 |
Primary Infections of the Skin |
285 |
Siderosis |
520 |
Complications Peculiar to Medical Care |
160 |
Contusion, Crushing, Bruise |
184 |
Other Skin Conditions |
286 |
Silicosis |
500 |
Effects of Changes in Atmospheric |
170 |
Cut, Laceration, Puncture |
185 |
Dermatitis, Allergenic or Contact |
287 |
Other Pneumoconioses |
|
Pressure |
190 |
Dislocation |
189 |
Skin Condition, NEC** |
289 |
Pneumoconiosis and Tuberculosis |
240 |
Effects of Environmental Heat |
200 |
Electric Shock, Electrocution |
|
Poisoning Systemic |
|
Nervous System, Conditions of |
220 |
Effects of Exposure to Low Temperature |
210 |
Fracture |
270 |
Poisoning, Systemic, UNS* |
560 |
Nervous System, Conditions of - NEC** |
530 |
Eye, other Diseases of the Eye |
250 |
Hernia, Rupture |
271 |
Due to Toxic Materials other than Lead |
561 |
Diseases of the Central Nervous |
230 |
Hearing Loss or Impairment |
300 |
Scratches, Abrasions |
272 |
Diseases of the Blood and Blood Forming |
|
System |
991 |
Heart Condition ,Excludes Heart Attack |
310 |
Sprains, Strains |
|
Organs |
562 |
Diseases of the Nerves and Peripheral |
320 |
Hemorrhoids |
400 |
Multiple Injuries |
273 |
Upper Respiratory Conditions |
|
Ganglia |
330 |
Hepatitis, Serum and Infective |
900 |
No Injury |
274 |
Influenza, Pneumonia, Etc. |
|
Neoplasm Tumor |
275 |
Hepatitis, Toxic |
950 |
Damage to Prosthetic Devices |
276 |
Other Diseases of the |
550 |
Neoplasm Tumor, UNS* |
260 |
Inflammation of Joints, Etc. |
995 |
No Other Injury, NEC** |
|
Tract |
551 |
Malignant |
540 |
Mental Disorders |
999 |
278 |
Effects of Lead |
552 |
Benign |
900 |
No Illness |
|
|
Infective or Parasitic Disease |
279 Other Toxic Effects of One System Only |
|
Radiation Effects |
999 |
||
150 |
Infective or Parasitic Disease, UNS* |
Respiratory Systems, Conditions of |
290 |
Radiation Effects, UNS* |
990 |
Occupational Disease, NEC** |
|
151 |
Amebiasis |
570 |
Respiratory Systems, Conditions of |
291 |
580 |
Symptoms and |
|
152 |
Anthrax |
571 |
Upper Respiratory |
292 |
Microwaves |
|
|
153 |
Brucellosis |
572 |
Asthma, Influenza, Pneumonia |
293 |
Ionizing Radiation - |
|
|
154 |
Conjunctivitis and Opthalmia |
|
Pneumoconiosis |
294 |
Ionizing Radiation - Isotopes |
|
|
156 |
Tetanus |
280 |
Pneumoconiosis |
295 |
Welder’s Flash |
|
|
BODY PART AFFECTED CODES
Head |
160 |
Skull |
398 |
Upper Extremities, Multiple |
513 |
Knee(s) |
|
100 |
Head, UNS* |
198 |
Head Multiple |
400 |
Trunk, UNS* |
515 |
Lower Leg(s) |
110 |
Brain |
200 |
Neck & Cervical Vertebrae |
410 |
Abdomen, Internal Organs, |
518 |
Leg(s), Multiple |
120 |
Ear(s), UNS* |
UPPER EXTREMITIES |
|
Inguinal Hernia |
519 |
Leg(s), NEC** |
|
121 |
Ear(s), External |
300 |
Upper Extremities, NEC** |
420 |
Back |
520 |
Ankle(s) |
124 |
Ear(s), Internal |
310 |
Arm(s), UNS* |
430 |
Chest, Ribs, Breastbone, |
530 |
Foot or Feet, Not Ankle |
130 |
Eye(s), UNS* |
311 |
Upper Arm |
|
Internal Organs |
540 |
Toe(s) |
140 |
Face, UNS* |
313 |
Elbow(s) |
440 |
Hip(s)..,Pelvis, Organs and |
598 |
Lower Extremities, Multiple |
141 |
Jaw, Chin |
315 |
Forearm(s) |
|
Buttocks |
700 |
MULTIPLE PARTS |
144 |
Mouth and Throat (vocal chords, larynx) |
318 |
Arm(s), Multiple |
450 |
Shoulder(s) |
|
Applies when more than one major body part |
146 |
Nose |
319 |
Arm(s), NEC** |
498 |
Trunk, Multiple |
|
as been effected such as an arm and a leg |
148 |
Face, Multiple Parts |
320 |
Wrist(s) |
LOWER EXTREMITIES |
999 |
||
149 |
Face, NEC** |
330 |
Hand(s), Not Wrists or Fingers |
500 |
Lower Extremities |
|
mation to identify part of body effected. In- |
150 |
Scalp |
340 |
Finger(s) |
510 |
Leg(s), UNS* |
|
cludes damage to prosthetic devises. |
*UNS - UNSPECIFIED |
**NEC - NOT ELSEWHERE CLASSIFIED |
| Fact Name | Details |
|---|---|
| Form Purpose | This form is used to report injuries or fatalities that occur in the workplace. |
| Filing Requirement | Employers must file this form within 7 calendar days of being notified of an injury. |
| Governing Law | The form is governed by Massachusetts General Laws, Chapter 152. |
| Submission Method | The completed form should be mailed to the Department of Industrial Accidents. |
| Penalties for Non-Compliance | Failure to file may result in a fine of $100, as stipulated in M.G.L. Chapter 152, Section 6. |
| Information Required | Essential details include employee information, injury description, and employer data. |
| Employee's Return to Work | The form includes a section to indicate if the employee has returned to work after the injury. |
| Language Codes | A section exists for native language codes, facilitating communication for non-English speakers. |
| Form Revision Date | The current version of the form was revised in July 2010. |
Fire Department Complaint Form - Businesses must provide a detailed account of their hazardous processes, including the categories that apply, to align with state safety regulations.
To ensure safety and mitigate risks, it is crucial to understand the implications of a Hold Harmless Agreement in various activities. You can learn more about its specifics in this important Hold Harmless Agreement form guide.
Ma Form M-3 - The form outlines the requirements and documents needed to complete your request, guiding you through the preparation of your application.